
I often described my breast pain as the sensation that a tiny pastry chef living in the upper left quadrant of my boob had attached razor blades to her whisk and was spinning it above her head. Sometimes it felt more like I’d pulled a poker from the fireplace, shoved it into the side of my breast, and left it there. Occasionally, the feeling was more like rapid-fire lightning strikes targeting the largest lump in my boob; those sudden, repeated jolts were the most likely to elicit audible “arghhhs” from between my gritted teeth.
Though an exact start date for the pain escapes me, I know it was likely in 2015, around the same time a gynecologist remarked, “Ooh, you’ve got very lumpy breasts, huh?” during an annual exam. This doctor gave me the—for lack of a better term—“diagnosis” of fibrocystic breast disease. And while I don’t blame her for it, this was the start of about a decade of living with excruciating pain that I thought I’d have to deal with for most of my life.
The reason “diagnosis” is not a great way to describe finding out you have fibrocystic breast disease is because it actually isn’t a disease at all. It isn’t even an anomaly. “There’s nothing abnormal or disease-like about it,” says Amani Jambhekar, MD, a board certified surgeon and the medical director of surgical breast oncology at Christus St. Vincent in Santa Fe, who notes that the more accurate name “fibrocystic breast changes” is starting to catch on. In fact, although the exact percentage is hard to lock down for reasons I'll explain shortly, it's believed that most women have fibrocystic breast changes to some degree.
Fibrocystic breasts can contain any combination of fluid-filled cysts, solid masses like fibrosis (scar tissue) or fibroadenomas (benign tumors), or an overgrowth of cells around the milk ducts. They’re called “changes” because those lumps tend to come and go throughout a patient’s life, sometimes corresponding with their menstrual cycle, but more often, totally randomly. “Probably everyone has one [of these changes] somewhere in their breast,” says Dr. Jambhekar. Sometimes you can feel these lumps yourself; sometimes they’re so small or deep inside your breast that you can only detect them via imaging. For my part, I have a combination of lumps I can feel and ones I wouldn’t know existed if my doctors hadn’t pointed them out on my sonograms. My extreme pain radiated from one particular lump located in the 2 o’clock quadrant on my left breast.
“Fibrocystic disease is kind of a catchall term that people throw around,” says Marybeth Hans, senior certified physician assistant and co-leader of the high-risk breast program (BPREP) at the Brigham and Women’s Comprehensive Breast Center. “It could really just mean that [a patient’s breasts] are lumpy, bumpy, and tender.” Elisa Port, MD, a board certified breast surgeon and chief of breast surgery for the Mount Sinai Health system, agrees, calling it a “waste basket term” that covers what’s essentially a normal state, especially for premenopausal women. Hans says that fibrocystic changes tend to be flagged incidentally—an offhand comment during an exam, like I experienced—or discovered during some unrelated surgical procedure. As with many conditions that primarily affect women, the best guess science currently has for what causes fibrocystic breast changes is just “hormones.”
By now, most people have come to fear sentences that contain the words “lump” and “breast,” but the lumps that come as a part of fibrocystic breast changes do not inherently put you at a higher risk of cancer. Just because you have cystic and fibrous tissue popping up left and right does not mean that one day your body will definitely throw a malignant tumor in there, too. “The only danger is if someone develops a new lump and basically is complacent and writes it off to [a change in their existing fibrocystic breast tissue], but it ends up being a cancer,” says Dr. Port. (This mistake seems to be fairly rare: Hans says she’s only experienced it once in her 30 year career.)
While Dr. Port says the current national guidelines recommend against self exams as a method of breast cancer detection (which, for the record, she disagrees with: “No one would ever say, don't look at your skin and check for new spots”) for someone with dense, lumpy breasts, those self exams will help you become familiar with your baseline bumps, so you can let your doctor know about any new ones. Areas of concern will be screened more thoroughly than what you get with your regular mammograms (which you might get to experience before you hit your 40s, if you have the one-two punch of fibrocystic and dense breasts—meaning you have more fibrous and glandular tissue than fatty breast tissue—like me). As long as you’re getting those screenings, the current medical consensus is that you have no additional breast cancer risk to worry about if you have fibrocystic breast changes.
–
If you Google “treatment for fibrocystic breast disease,” the results you get on medical websites go something like this: Fibrocystic breast disease is a condition that doesn’t need to be treated, because it doesn’t cause symptoms…except when it causes breast pain. All the doctors I spoke to for this story told me that most people fall into the “no symptoms” category, though it’s hard to say exactly what percentage constitutes “most,” since people without symptoms might never even realize they have these changes. I, clearly, was not one of the “most.”
If your lumpy boobs hurt, the medical websites go on, it’s easy to fix that: Simply stop consuming any caffeine, alcohol, fatty foods, salty foods, or sugary foods (although the doctors I spoke with say some studies and plenty of anecdotal evidence show that, for some people, diet changes have no effect), wear a sports bra 24/7 (as in, every single day and also to bed), and perhaps try taking evening primrose oil supplements (although we’re pretty sure that one doesn’t actually work either). Over-the-counter painkillers like ibuprofen can help, though, as Hans and Dr. Jambhekar and my own primary care doctors have all told me, you really shouldn’t be taking those every day.
At various points over the past 10 years, I gave all of those at-home remedies a try. The sports bra thing did kinda work—the pain became more of a dull ache than a white-hot, burning sensation—but wearing a tight bra all the time sucks. I felt claustrophobic to the point of mild panic attacks when I wore them to bed, so I gave up.
The other potential cure for pain from fibrocystic breasts is to wait for menopause, when those lumps and any correlating breast pain go away for most people. This was the “solution” that I was offered most often, as if I should feel satisfied enough with the knowledge that the excruciating daily pain would (probably) go away if I just waited it out for a few decades.
—
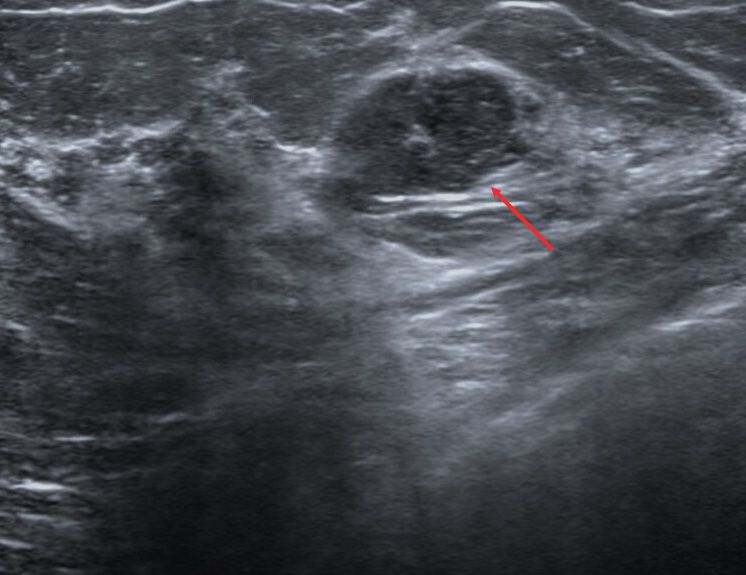
In 2019, I told my ob-gyn that I felt like my largest lump was getting bigger, so she ordered a mammogram, followed by the diagnostic sonogram that typically has to be ordered for people with dense breasts who feel a suspicious bump. Breast density is measured on a scale of A to D; Hans tells me that about 10% of women fall into the “A” category (mostly fatty tissue aka not dense), 10% into “D” (extremely dense), and the rest somewhere in the “B” and “C” range. The less dense your breasts are, the easier it is for a doctor to spot a mass sitting among your tissue: On X-ray imagery (including mammograms), tumors look white, while fatty tissue is gray. The tissue inside extremely dense breasts, like mine, are lighter in color, making those tumors harder to spot unless you’re really looking for it via a targeted sonogram. Simple cysts and fibroadenomas show up as black holes amongst the lighter tissue, which I have to say look terrifying, despite their benign nature.
Even though my lump seemed to be of the crisp black hole variety, my doctor also ordered a biopsy because I was concerned it was growing. That biopsy hurt like hell despite the local anesthetic. But! No cancer. I felt (and still feel) so grateful that I once again resigned myself to living with my bundle of painful cysts until I hit menopause. If it was such a common condition, that meant millions of other people were doing the same thing. I could suck it up and deal just like they were.
That is until one day in the summer of 2024, when my boob was throbbing and I was feeling particularly cranky about the fact that I and other people with this type of pain are supposed to just live with it. Since I am in the unique position of working at a website with millions of predominantly female readers, I pitched the idea of doing a story about fibrocystic breast changes. I envisioned a fairly straightforward explainer that rounded up everything we know about the condition so far and called for more research into what causes it and how patients could better manage their symptoms. It would be cathartic for me to write about this extremely common condition and, I hoped, helpful for everyone else who was dealing with it, even if only so they knew they weren’t the only ones.
During my phone interviews with Hans, Dr. Jambhekar, and Dr. Port, I asked them all if there had been any new discoveries made about treating the pain associated with fibrocystic breast changes. All three of them said essentially the same thing: Pain associated with fibrocystic breast changes is pretty rare (yes, so I have heard) and those at-home remedies tend to provide mediocre-at-best-results, but if you do have a really painful cyst, you can have it drained, which usually provides instant relief.
“But I have a really painful cyst that hurts all the time, and no one has ever offered to aspirate it,” I said to Hans, the first expert I spoke with, after apologizing for asking a personal question rather than one for the story. “They just went straight to a core biopsy and when it came back negative, I was told there was nothing to worry about.”
Hans paused, then explained that doctors wouldn’t be able to do a core biopsy on a cyst. “As soon as you put the core biopsy device in there, it would just drain on you,” she said. “Simple cysts are just pure fluid.” And that’s when I realized I was totally mistaken about what was going on in my boobs.
—
I know it’s not a good idea to ask a medical professional who has never seen you in person to diagnose you over the phone, but I ended up telling all three experts about my own symptoms and they agreed I probably wasn’t dealing with a cyst. So, at my annual physical a few months later, I told the nurse practitioner doing the exam about my ongoing pain and what I’d learned in the interviews and she consented to refer me to the breast department. A few weeks later, I had another mammogram and sonogram combo, then met with a surgeon. He told me that my lump was, in fact, a fibroadenoma—or non-cancerous breast tumor—and said that he could remove it but that doing so wouldn’t necessarily get rid of the pain.
The majority of people with breasts will experience breast pain, but the cause is typically unclear. “A lot of women who have breast pain don't have that actual fluid-filled cyst that you can find on imaging,” Hans says. “Most times, we come up empty. We do not find a lesion and say, ‘Oh, this is what’s hurting you.’” Although I did have a lump that seemed to correspond with where the pain was coming from, that could have been totally coincidental. My surgeon repeated the same line I’d heard from so many people and medical websites: Fibroadenomas don’t usually cause pain.
Still, because the lump seemed tender to the touch and my medical history meant I had a low risk of negative side effects during or after the surgery, we both thought it was worth a shot. I scheduled the surgery for the Monday after my 35th birthday and took the three days following the procedure off of work. In the two months between that consultation and the surgery, I learned it was easier to be specific with people who asked about the procedure: If I said I was having a lump removed (versus a benign fibroadenoma), they panicked.
The surgery—as far as I, a person whose only other surgery has been to have some baby teeth that were fused to my jawbone removed, can tell—went smoothly. The worst part was having to use that nasty pink soap (if you’ve had an operation, you know the soap I mean) and no other beauty products for the 24 hours before the appointment. I was awake on the operating table until I wasn’t; I came to with a jolt about an hour later wearing a purple surgical bra that I despised for the entire 48 hours I could stand to wear it, at which point I switched to a sports bra with my surgeon’s permission.


Once I was home and healing, I finally understood how bad my pain from the fibroadenoma had been. The surgeon prescribed opioids to manage the post-surgery healing process, but I never even took a Tylenol. The pain from the incision was nothing compared with what I’d been living with for about a decade—and that pain was completely gone. The devilish pastry chef had been 86’d.
I’m writing this almost exactly five months after the surgery and am thrilled to report I’m still completely pain free in the boob department, a fading one-inch scar the only reminder of the bothersome lump. I asked my surgeon at the follow up appointment if he’d seen anything inside my breast that indicated why this particular fibroadenoma had been giving me so much trouble and he shrugged. “Nope,” he said. “I was expecting to see it pushing on a huge bundle of nerves or something, but there was nothing there.”

There are a lot of stories of women being ignored or dismissed at the doctor’s office, their symptoms downplayed until they end up in the emergency room with a brain aneurysm or metastatic cancer or a burst appendix. That’s not what I experienced. Every doctor I spoke to nodded sympathetically as I described my symptoms. They totally understood that breast pain is very real and very common. But they also seemed to believe that, because it was normal and didn’t seem to be connected to anything that would kill me, there was no way or no reason to treat it. Since that’s the message I was taking away from the appointments, I believed that the majority of women were walking around feeling the same way I did and I didn’t hear them complaining, so I shut my mouth.
When I tell people about my experience, many of them can’t quite wrap their heads around why there aren’t more pain management options for people with breast pain—whether it’s from a fibroadenoma or cyst or of some mysterious origin. “If this was random testicle pain,” one of my editors (a man himself) said, “there would be free ibuprofen dispensers in every men's room.” The three doctors I spoke to all seemed frustrated by the lack of medical consensus over how to treat a condition that affects the vast majority of women.
“I think sometimes women feel a little bit dismissed by their primary care provider or ob-gyn, probably because those doctors know that [breast pain] is common. They see it all the time,” says Hans. “They think it's reassuring to tell somebody that it’s nothing or it's normal. But the patient is like, ‘Wait, but I'm looking for more of an explanation.’”
I technically still don’t have a precise explanation myself, but I do know that my pain is gone. I don’t recommend everyone with lumpy, hurting boobs go in and demand a similar surgery, but I do want you to know it’s an option—and you should demand to know all your options, especially as research around the phenomenon (hopefully) continues to grow. “I definitely don't think that the answer is that women should just walk around and continue to be uncomfortable,” Dr. Jambhekar says. “Women deserve better options.”
Read more first-person stories:
The Wellness Industry Has No Use for My Cancer Diagnosis
A $10,000 Surgery Gave Me Perfect Vision–and a New Vanity
I Tried Everything to Treat My Hair Loss
Follow Allure on Instagram, TikTok, and Substack, or subscribe to our newsletter to stay up to date on all things beauty.












